What is an Ankle-Brachial Index (ABI)?
An ABI test is a simple, reliable test for diagnosing PAD in the legs. The test measures the blood pressure in your ankles and compares it to that in your arms. If the blood pressure is lower in your legs than in your arms, it may indicate that PAD is restricting blood flow in your legs. The ABI test is fast and painless, and does not require entering the body.
In some cases, the ABI test may be performed after exercise on a treadmill, called an exercise ABI. The exercise ABI can diagnose PAD in women who have PAD symptoms during exercise, but a normal ABI measurement at rest. In the early stages, PAD may only cause symptoms when the leg muscles are working hard and need more blood than usual. See Exercise Tests for more detailed information.
Who might have an ABI test?
Because it is simple, reliable, and safe, the ABI test is usually the first test used to diagnose PAD in women who have PAD symptoms such as leg discomfort, numbness, or nonhealing sores.
The ABI is also used to look for PAD in women who do not have any symptoms, but are at risk for the disease because they have risk factors for PAD. See PAD Screening to find out if you should be tested for PAD, and to find a screening site near you.
In women who have already been diagnosed with PAD, the ABI can monitor how severe your PAD is and help predict whether wounds will heal on their own. After a procedure to open leg arteries such as angioplasty, stenting, or lower-extremity bypass surgery, an ABI can indicate how effective the treatment was at improving blood flow in the leg.
Who should not have an ABI test?
Women who have a suspected blood clot in the veins of the legs (deep vein thrombosis, or DVT) should not have an ABI test. Because the ABI involves squeezing the leg with a blood pressure cuff to stop blood flow, it could cause a clot in the leg veins to break off and travel to the lungs, causing a potentially deadly pulmonary embolism. For this reason, an ultrasound should be used to rule out DVT before performing an ABI in women with suspected blood clots in the veins.
How do I prepare for the test?
You should not smoke or participate in strenuous activities for 24 hours before the test. You should take any medications and eat and drink as you normally would.
What happens during an ABI test?
The ABI test is simple and painless, and takes about 15 minutes. It can be performed in your doctor’s office or at specialized testing center.
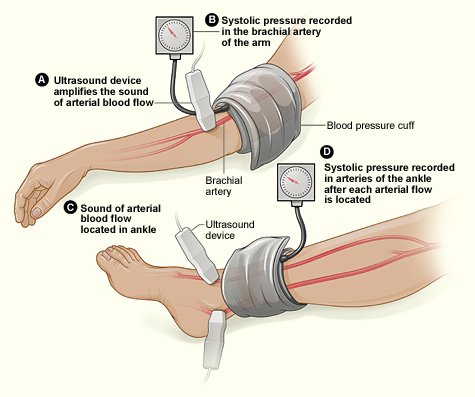
You will lie on your back on a table. A technologist will place a blood pressure cuff on your upper arm, and it will be inflated until blood flow through the brachial artery (which runs down the inside of your upper arm) stops. As the cuff is slowly deflated, the doctor will measure your systolic blood pressure (the top number in a normal blood pressure measurement) using a hand-held device called a Doppler probe placed near the crease of your elbow. The probe is a pen-like device that is pressed lightly against your skin and uses reflected sound waves to accurately measure blood pressure. The technologist will apply a bit of gel to your skin before using the probe to help the sound waves travel better. This process will be repeated with the other arm.
Then the technologist will measure your blood pressure in each leg. The doctor will feel for the pulse in the artery that runs down your leg over the top part of your foot. A blood pressure cuff just above your ankle will be inflated and slowly deflated, and the Doppler probe will be used to measure blood pressure. This will be repeated for the artery on the inside of your ankle.
What do the results mean?
Your ABI number is calculated by taking the systolic (top number) blood pressure in your ankle and dividing by the blood pressure in your arm. When the blood pressure readings are different between your left and right arm, the higher of the two numbers is used.
A low ABI means the blood pressure in your legs is lower than that in your arms, indicating that PAD is restricting blood flow to your legs. The lower your ABI number, the more severe your PAD is. Women with a lower ABI are more likely you are to suffer complications of PAD such as foot ulcers and walking limitations.1,2
A low ABI score also indicates you are at risk for other forms of artery disease, including coronary artery disease. In one large study, women with an ABI of 0.90 or less were 3.5 times as likely to die of heart disease within 10 years compared with women with a normal ABI.3
Ankle-Brachial Index (ABI) Results4
| ABI Number | Diagnosis | What It Means |
| 1.00 to 1.29 | Normal | Your ABI is in the normal range and you are not likely to have PAD. |
| 0.91-0.99 | Borderline | Your ABI is slightly lower than normal, but not low enough to diagnose PAD. Your doctor may want to measure your ABI again soon to make sure it is not getting worse, or measure your ABI after exercise. |
| 0.41 to 0.90 | Mild-to-moderate PAD | You have PAD. Working with your doctor to get your risk factors under control can prevent the disease from getting worse, and treatments are available to help relieve your PAD symptoms. |
| 0.40 or less | Severe PAD | The blood flow in your legs is severely obstructed, and you may need immediate treatment to relieve your symptoms and prevent serious complications. |
An ABI higher than 1.3 indicates that the arteries in your legs are stiff and cannot be closed off by the blood pressure cuff, causing an inaccurate reading. This often happens in elderly women and women who have had diabetes for many years or who are on dialysis for chronic kidney disease.
If your arteries are too stiff to get an accurate ABI reading, you will need another test to diagnose PAD, such as a toe-brachial index (TBI), pulse volume recording, or ultrasound.
How reliable is the ABI test at detecting PAD?
The ABI is one of the most accurate tests for diagnosing PAD in the legs. Studies have shown that the ABI can identify about 90% of women with PAD, and fewer than 5% of women with a low ABI turn out not to have PAD.5,6
Women tend to have slightly lower ABI numbers than men do. One study of 1,775 healthy people (58% were women) found that, on average, women had ABIs that were 0.02 lower than men’s.7 However, there is no evidence that the ABI test is less accurate for diagnosing PAD in women compared with men, or that different ABI cutoffs should be used for women.
What are the risks of an ABI test?
The ABI test is generally safe and painless, and does not require entering the body. You may feel some discomfort as the blood pressure cuff inflates to cut off blood flow.
If you have blood clots in the veins (DVT), the squeezing of the blood pressure cuff during an ABI test could cause the clot to break off and travel through the bloodstream. If the clot becomes lodged in another blood vessel this can cause serious complications, such as a potentially deadly pulmonary embolism. For this reason, an ultrasound should be used to rule out DVT before performing an ABI in women with suspected blood clots in the veins.
What happens next?
If your ABI number indicates you may have PAD, you may need more tests to examine blood flow in your leg arteries if a procedure is planned. If you have only mild-to-moderate PAD, you doctor may decide to start you on a treatment plan and check your ABI again if your symptoms get worse.
If your ABI is lower than normal but not yet low enough to diagnose PAD (a borderline result), your doctor may want to check your ABI after exercise (see exercise tests for more).
Other tests that may be used to further investigate PAD include:
- Functional tests to provide additional information about blood flow:
- Tests that produce pictures of the shape of the arteries and blood flow through them:
Related Tests
What is a segmental pressure measurement test?

A segmental pressure test is performed in the same way as an ABI test, except that additional blood pressure cuffs are used to take measurements in different parts of the leg. Usually the test uses four cuffs, placed on the upper thigh, lower thigh, upper calf, and just above the ankle, with blood pressure measurements taken at each point.
Segmental blood pressure measurement.
The segmental blood pressure test is used to get a better idea of where a blockage or narrowing your leg arteries is located. If the blood pressure drops more than about 20 mm Hg between one cuff and the next, it is likely that the blockage is located in between those two cuffs.4
Like an ABI, segmental pressure measurement may be used to diagnose PAD or determine the effectiveness of PAD treatments. While the ABI can only tell whether or not you have PAD, segmental blood pressure measurement can also show approximately where the blockage is located. This information may be used to predict whether sores on the leg will heal based on their location, or to help formulate a PAD treatment plan. If doctors need to know the exact location or extent of a blocked artery, they may use a more detailed test such as ultrasound, an MR angiogram, a CT angiogram, or a contrast angiogram.
What is a toe-brachial index test?
A toe-brachial index test (TBI) is nearly identical to an ABI test, except instead of measuring the blood pressure in your ankle, a tiny blood pressure cuff and sensor are used to measure the blood pressure in your big toe.
A TBI test is often used to diagnose PAD in women whose leg arteries are too stiff to get an accurate ABI result (an ABI more than 1.3). The TBI is more accurate in these women because the arteries in the toe are usually not as stiff as those in the leg. A TBI of 0.7 or less usually means you have PAD. The TBI is also useful for predicting whether wounds on the foot or toe will heal.
References
- Allison MA, Hiatt WR, Hirsch AT, Coll JR, Criqui MH. A high ankle-brachial index is associated with increased cardiovascular disease morbidity and lower quality of life. J Am Coll Cardiol. Apr 1 2008;51(13):1292-1298.
- McDermott MM, Criqui MH, Liu K, et al. Lower ankle/brachial index, as calculated by averaging the dorsalis pedis and posterior tibial arterial pressures, and association with leg functioning in peripheral arterial disease. J Vasc Surg. Dec 2000;32(6):1164-1171.
- Ankle Brachial Index Collaboration. Ankle Brachial Index Combined With Framingham Risk Score to Predict Cardiovascular Events and Mortality: A Meta-analysis. JAMA. July 9, 2008 2008;300(2):197-208.
- Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. Mar 21 2006;113(11):e463-654.
- Fowkes FG. The measurement of atherosclerotic peripheral arterial disease in epidemiological surveys. Int J Epidemiol. Jun 1988;17(2):248-254.
- Feigelson HS, Criqui MH, Fronek A, Langer RD, Molgaard CA. Screening for peripheral arterial disease: the sensitivity, specificity, and predictive value of noninvasive tests in a defined population. Am J Epidemiol. Sep 15 1994;140(6):526-534.
- Aboyans V, Criqui MH, McClelland RL, et al. Intrinsic contribution of gender and ethnicity to normal ankle-brachial index values: the Multi-Ethnic Study of Atherosclerosis (MESA). J Vasc Surg. Feb 2007;45(2):319-327.
- Kaufman JL, Fitzgerald KM, Shah DM, Corson JD, Leather RP. The fate of extremities with flat lower calf pulse volume recordings. J Cardiovasc Surg (Torino). Mar-Apr 1989;30(2):216-219.
- Symes JF, Graham AM, Mousseau M. Doppler waveform analysis versus segmental pressure and pulse-volume recording: assessment of occlusive disease in the lower extremity. Can J Surg. Jul 1984;27(4):345-347.


